ANKLE LIGAMENT REPAIR
…the brostrum gould procedure….
WHAT ARE THE ANKLE LIGAMENTS?
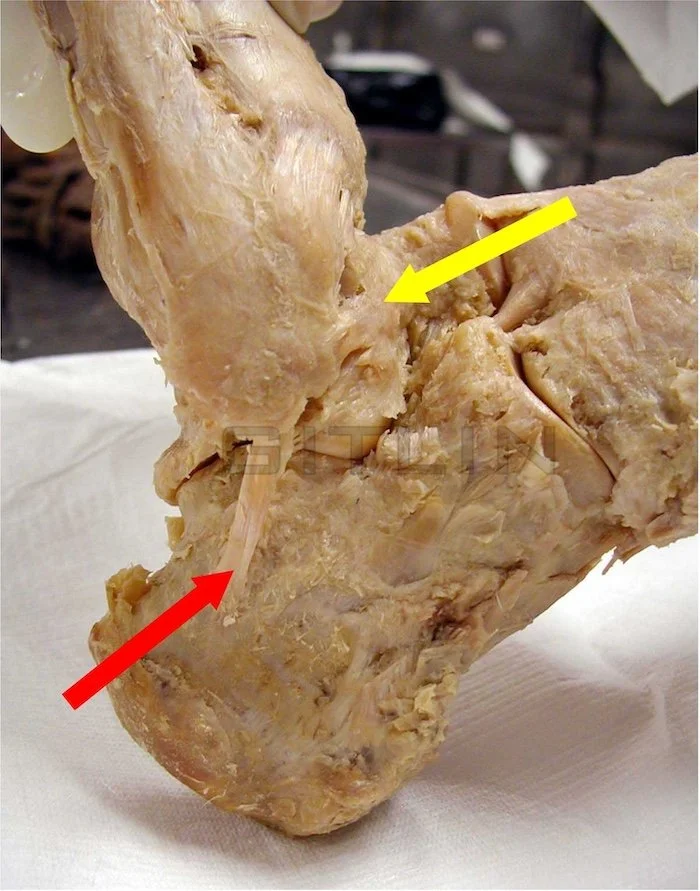
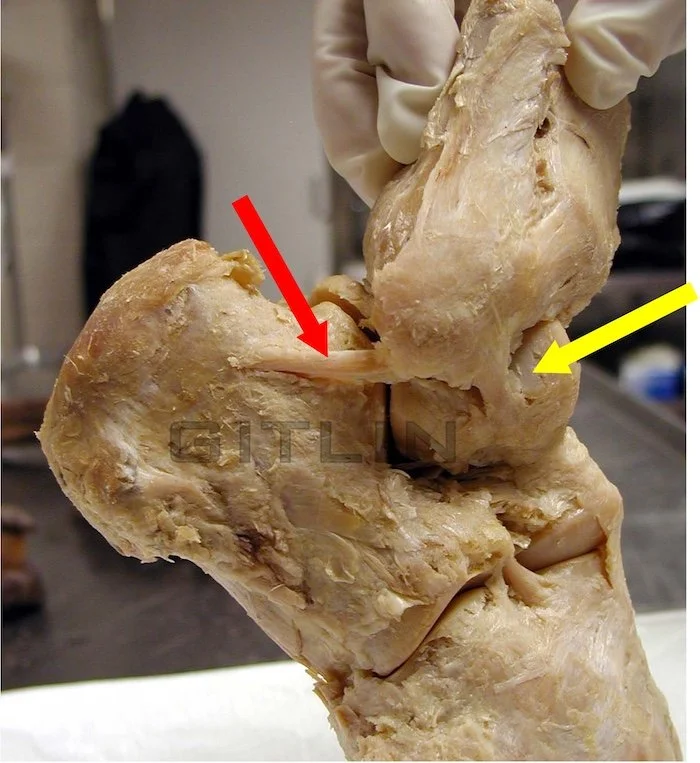
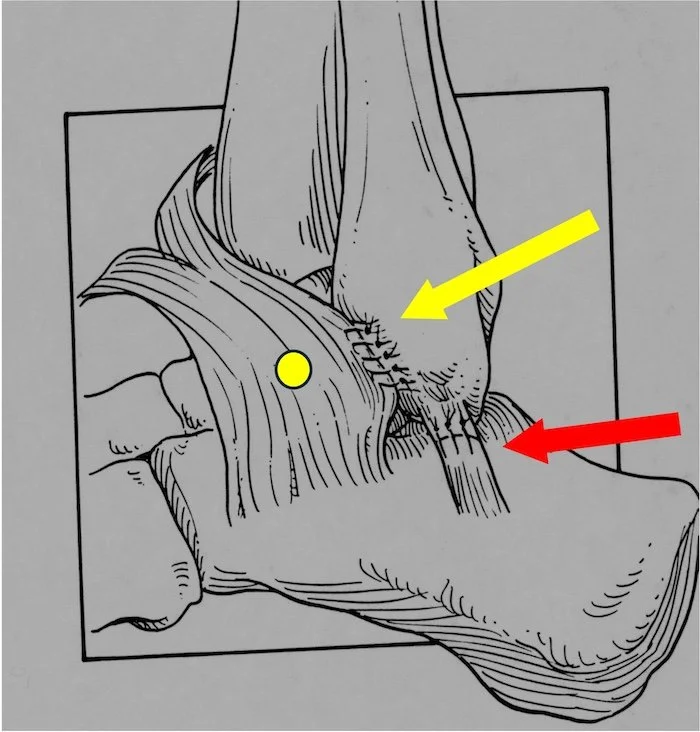
Bones that make up a joint need to have some way to attach to each other and still allow for some motion. Structures that resemble tight rubber bands perform this function and are called the ligaments. ( the word comes from Latin word ‘to bind together’) Joints can have many of these ligaments holding the bones together, in the ankle there are these structures on all sides of the joint. The ones that are most often injured are the ones on the outside of the ankle. These are called the Anterior Talo-fibular ligament ( ATFL) and the Calcaneo-fibular ligament (CFL). If you look at the name it tells you which bones they connect , the ATFL connects the talus (foot bone) to the fibula (the outer ankle bone). These ligament not only hold together the bones but also function to limit joint motion. So - when they are torn a patient can have instability in the ankle. In the pictures below a cadaver is shown and the red arrow points to the CFL while the yellow to the ATFL.
HOW DO THE ANKLE LIGAMENTS GET INJURED?
One of the most common injuries in the body is the ankle sprain. There is estimated that there are over 2 million ankle sprains every year in the United States. If you really want to know more you can click the link below, otherwise keep reading here.
The way an ankle usually rolls is inward, we call that an inversion ankle sprain. Depending on how far the ankle turns will determine what structure is injured. In some cases the ligament get stretched out in other cases one or two of the ligaments can get torn. Generally the ATFL tears first as the ankle twists because of its function and anatomic position. If the ankle continues to roll inward the CFL ligament will then tear. The treatment is dictated by the extend of the injury.
WHAY ARE THESE LIGAMENTS SO IMPORTANT?
It is known in the medical literature that the ankle ligaments contain nerve sensors that communicate with the brain. These are called proprioceptive sensors since they convey information on position of the ankle during walking. Patients who had an ankle sprain injury tend to walk slower and mare more adjustments to their walking patterns. Here is a link to a recent medical journal article if you want to know more, otherwise keep reading.
HOW DO WE TEST ANKLE TO SEE IF ITS UNSTABLE AND MAY NEED SURGERY?
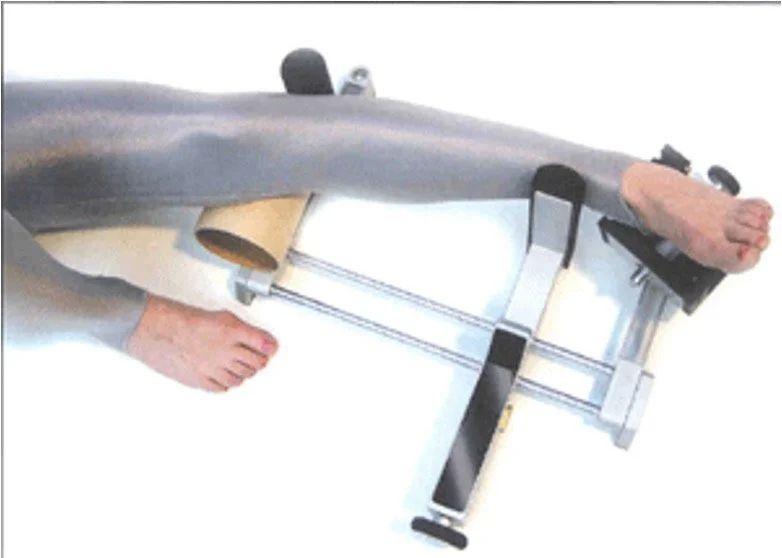
We sometimes do simple test called stress tests to see how much slack the ligaments have and how much they allow the ankle to give way. sometimes its obvious, other times its not so much. Then we may do these tests under an X-ray machine for with a TELOS device that stresses an ankle for us in a specific direction. there tests are called the talar tilt test and the anterior draw test. Both are done to assess ankle ligament strength.


HOW DO WE FIX IT IF IT DOESN’T HEAL WITH CONSERVATIVE TREATMENT?
Initially the treatment is the regular rest, ice , elevation and possibly immobilization. Occasionally casting and nonweight bearing are used as treatment but again that depends on the severity of the injury. Physical therapy to strengthen surrounding structures around the joint are sometimes suggested. Even with the best initial conservative care sometimes the pain and instability just do go away. In these cases we may consider surgical repair.
WHAT IS THE SURGERY THATS IS DONE TO TREAT LATERAL ANKLE INSTABILITY ?
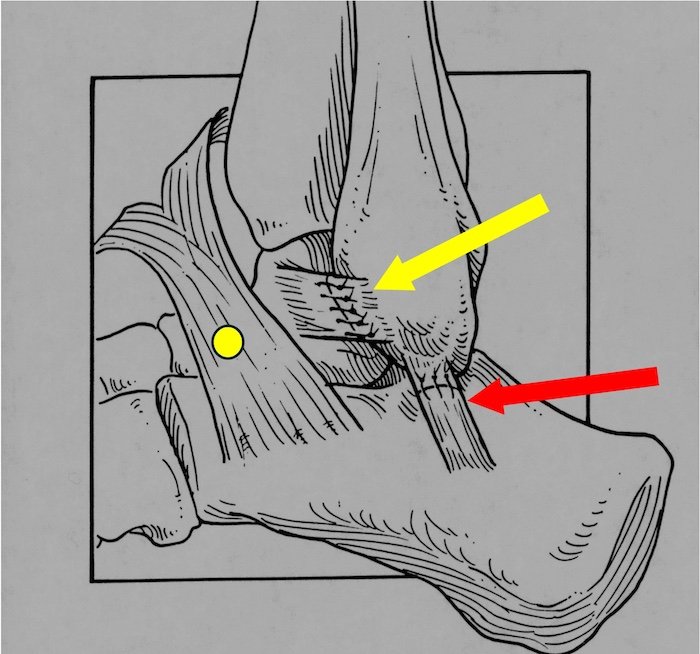
The most common procedure we do for this is called the Brostrum Gould procedure. Here we tighten the ATFL ligament by removing a small section of it and sewing it closed and tightened. In the picture below you can see this pointing with the yellow arrow. Then we take take a structure called the extensor retinaculum marked in the picture by the yellow dot and sew it into the already repaired ATFL to strengthen the repair. This is a vital step to a predictable result. The red arrow points to a repaired CFL ligament, in some cases this does need to be done as well.
What is the damage is too severe for that procedure; is there any other treatment?
Yes there is , another surgical procedure that we do is called a Christman Snook Tendon transfer. Here we take a tendon graft and replace the ligaments with a piece of tendon. In this case we drill holes in the bones and use tendon anchor implants to secure everything together. I won’t go into this here, we do not often need to do this procedure and it does deserve a separate full page. I typically use it when a patient already had a brostrum gould that did not give the desired outcome.
More general info below if you want to read but the above is the basic information a patient needs to understand the procedure. By the way i did mention something called a retinaculum. That is not a figment , it is a soft tissue structure that the body has to keep pus streamlined. In other words it keeps at the muscles , tendons and sometimes arteries and nerves tight up again the bones deep. We use these structures on occasion in multiple other surgical procedures to tighten things against the bone.
Brostrom-Gould Procedure: Surgical Solution for Chronic Ankle Instability
Introduction:
Chronic ankle instability, a debilitating condition characterized by recurrent ankle sprains and a feeling of "giving way," significantly impacts quality of life. The Brostrom-Gould procedure offers a surgical solution to repair damaged lateral ankle ligaments, restoring stability and function. This article provides a comprehensive overview of the Brostrom-Gould procedure, its indications, surgical techniques, recovery process, and potential complications.
Understanding Chronic Lateral Ankle Instability (CLAI):
Chronic Lateral Ankle Instability (CLAI) occurs when the lateral ankle ligaments, primarily the Anterior Talofibular Ligament (ATFL) and Calcaneofibular Ligament (CFL), fail to heal properly after an ankle sprain. This leads to:
Recurrent Ankle Sprains: Frequent ankle "give-way" incidents.
Persistent Ankle Pain: Chronic pain on the lateral ankle.
Ankle Swelling and Inflammation: Ongoing inflammatory responses.
Ankle Instability Symptoms: Subjective feeling of ankle looseness.
Proprioceptive Deficits: Reduced ankle position awareness.
Brostrom-Gould Procedure Indications:
This procedure is recommended for patients with:
Chronic Ankle Instability (CLAI) Treatment Failure: Non-surgical interventions like physical therapy, bracing, and activity modification have proven ineffective.
Lateral Ankle Ligament Tears: MRI or physical examination confirms ATFL or CFL ligament laxity.
Impactful Ankle Instability: Daily activities and quality of life are compromised by persistent ankle instability.
Brostrom-Gould Surgical Technique:
The Brostrom-Gould procedure repairs and reinforces lateral ankle ligaments:
Anesthesia Administration: General or regional anesthesia.
Lateral Ankle Incision: Small incision for access.
Ligament Identification (ATFL, CFL): Identification of damaged ligaments.
Lateral Ankle Ligament Repair: Sutures tighten and repair torn ligaments.
Gould Augmentation Technique: Reinforcement using surrounding tissue or grafts.
Surgical Closure: Incision closure and sterile dressing.
Ankle Immobilization: Splint or brace application.
Brostrom-Gould Procedure Recovery:
Post-operative recovery involves:
Ankle Immobilization Period: Several weeks for ligament healing.
Post-Operative Pain Management: Medication for discomfort.
Ankle Swelling Reduction: Ice and elevation techniques.
Ankle Rehabilitation (Physical Therapy): Restoring range of motion, strength, and proprioception.
Gradual Weight-Bearing Progression: Following surgeon's protocol.
Return to Activity Timeline: Several months for full recovery.
Brostrom-Gould Procedure Complications:
Potential risks include:
Surgical Site Infection: Infection risk post-surgery.
Post-Operative Bleeding: Bleeding during or after the operation.
Ankle Nerve Damage: Potential damage to surrounding nerves.
Ankle Joint Stiffness: Post-operative stiffness.
Recurrent Ankle Instability (CLAI): Ligament re-tear or stretching.
Wound Healing Issues: Problems with incision healing.
Complex Regional Pain Syndrome (CRPS): Rare chronic pain complication.
Conclusion:
The Brostrom-Gould procedure is a viable surgical option for chronic lateral ankle instability, restoring stability and function. Consult with a specialist to determine suitability.
FREQUENTLY ASKED QUESTION ON ANKLE INSTABILITY SURGERY
1. What is a Brostrom‑Gould ankle ligament repair?
A Brostrom‑Gould repair is a surgical procedure to tighten and repair the lateral ankle ligaments (usually the ATFL and often the CFL) when they have been stretched or torn from repeated ankle sprains. The ligaments are shortened and reattached to bone, and then reinforced with nearby tissue (the Gould augmentation) to restore stability to the outside of the ankle. The goal is to reduce the ankle “giving way,” prevent further sprains, and protect the joint from long‑term damage.
2. Who is a good candidate for Brostrom‑Gould surgery?
This surgery is usually recommended for patients who:
Have chronic ankle instability (repeated sprains, feeling of “giving way”)
Have already tried non‑surgical treatment such as bracing, physical therapy, and activity modification for several months without enough improvement
Have exam and/or MRI findings showing laxity or tears of the lateral ligaments
Are limited in sports, work, or daily activities because of instability
Patients with very generalized ligament laxity, severe arthritis, or major deformity sometimes need a different or more complex reconstruction, which is decided on a case‑by‑case basis.
3. How long is the recovery after Brostrom‑Gould ankle ligament repair?
Recovery is typically several months, and is staged:
First 2–4 weeks: The ankle is usually protected in a splint or cast. Weight‑bearing is limited or non‑weight‑bearing to let the ligaments heal.
Weeks 4–6 (approximate): Transition into a boot and begin gentle range‑of‑motion exercises if the repair is healing well.
Weeks 6–12: Progress to more full weight‑bearing, strengthening, and balance (proprioception) work in physical therapy.
3–6 months: Gradual return to higher‑impact activities such as running, cutting, and pivoting sports, depending on progress, sport demands, and your surgeon’s protocol.
Full healing and confidence in the ankle can continue to improve for up to a year.
4. When can I return to sports or full activity after Brostrom‑Gould surgery?
Most patients can expect:
A return to light activities (walking on even surfaces, stationary bike, basic gym work) between 6–8 weeks, depending on healing and pain.
A gradual return to running and higher‑impact activity over 3–4 months, once strength, range of motion, and balance are adequate.
A return to cutting and pivoting sports (soccer, basketball, tennis, etc.) at around 4–6 months, sometimes longer for high‑demand athletes.
The exact timing depends on your healing, pre‑injury level, and how demanding your sport or job is. Rushing back too early can risk stretching out the repair.
5. What are the risks and possible complications of Brostrom‑Gould ankle ligament repair?
As with any surgery, there are risks. Possible complications include:
Infection or wound‑healing problems at the incision site
Nerve irritation or numbness around the outside of the ankle or foot
Stiffness or reduced motion in the ankle
Persistent or recurrent instability if the ligaments stretch out again or if the tissues are very lax
Painful scar tissue or nerve sensitivity
Very rarely, complex regional pain syndrome (CRPS), a chronic pain condition
Most patients do well and have improved stability and fewer sprains when they follow the post‑operative and rehabilitation plan closely.
You can use the form below to email us directly, it is not HIPPA compliant meaning this information is not guaranteed secure and private. Don’t use your full last name just initial.
Our Florida and New York Office Locations
NAPLES OFFICE (Gulf Coast)
Serving Southwest Florida, including Fort Myers, Cape Coral, Bonita Springs, and Sarasota.
Address: 3940 Radio Road, Unit 104, Naples, FL 34104
Phone: 239-465-0311
WESTON OFFICE (Atlantic)
Serving the Tri-County area, including Miami, Boca Raton, West Palm Beach, and Hollywood.
Address: Weston near Cleveland Clinic coming soon
Phone: 239-465-0311
NEW YORK CITY OFFICE
Serving New York City and the boroughs as well as the entire Tri-state area
Address: 330 W. 58 street, Unit 610, NYC, NY 10019
Phone: 212-372-0991